Chance News 78: Difference between revisions
(Undo revision 14300 by Bill Peterson (talk)) |
|||
| Line 61: | Line 61: | ||
==Saw palmetto and LUTS== | ==Saw palmetto and LUTS== | ||
As most older men will attest, lower urinary tract symptoms or LUTS in the form of BPH or benign prostatic hyperplasia, is at minimum annoying, and often quite painful. The most common plant extract for treating BPH is the fruit of the saw palmetto dwarf palm tree. Saw palmetto is relatively inexpensive, around 20 to 30 dollars for a so-called month supply and according to [http://www.sawpalmetto.com/lib/proscar.html The Saw Palmetto Trading Company] | |||
<blockquote> | |||
Numerous double-blind clinical studies on the Saw palmetto extract have shown it to be effective in nearly 90% of patients usually in a period of 4 to 6 weeks. Detailed toxicity studies in animals, as well as the results from clinical trials, indicate that the Saw palmetto extract is without toxicity or side effect. Despite the impressive clinical effectiveness, safety, and popularity of Saw palmetto extract in the treatment of BPH in the United States, manufacturers are prohibited from making any medical claims by the FDA. | |||
</blockquote> | |||
Clinical studies demonstrating the efficacy of Saw palmetto in BPH: | |||
{| class="wikitable" | |||
|- | |||
! Authors | |||
! Type of Study | |||
! No. of patients | |||
! Length of study | |||
! Results | |||
|- | |||
| Boccafoschi, et al | |||
| Double-blind | |||
| 22 | |||
|60 days | |||
|Significant difference for volume voided, maximum flow, mean flow, dysuria, nocturia | |||
|- | |||
| Cirillo,et al | |||
| Open | |||
| 47 | |||
| 4 months | |||
| Significant difference for: dysuria, nocturia, urine flow | |||
|- | |||
| Tripodi, et al | |||
| Open | |||
| 40 | |||
| 30-90 days | |||
| Significant difference for: dysuria, nocturia, volume of prostate, voiding rate, residual urine | |||
|- | |||
| Emili, et al | |||
| Double-blind | |||
| 30 | |||
| 30 days | |||
| Significant difference for: number of voidings, strangury, maximum and mean urine flow, residual urine | |||
|- | |||
| Greca, et al | |||
| Open | |||
| 14 | |||
| 1 to 2 months | |||
| Significant difference for: dysuria, perincal heaviness, nocturia, volume of urine per voiding, interval between two dumal voidings, sensation of incomplete voiding | |||
|- | |||
| Duvia, et al | |||
| Controlled trial vs. pygeum | |||
| 30 | |||
| 30 days | |||
| Significant difference for voiding rate | |||
|- | |||
| Tasca, et al | |||
| Double-blind | |||
| 30 | |||
| 31 to 90 days | |||
| Significant difference for: frequency, urine flow measurement | |||
|} | |||
However, [http://jama.ama-assn.org/content/306/12/1344.short a recent JAMA study] indicates that a popular remedy for LUTS might be worthless: | |||
<blockquote> | |||
In conclusion, we found that saw palmetto extract used at up to 3 times the standard daily dose had no greater effect than placebo on improving lower urinary symptoms or other outcomes related to BPH. | |||
</blockquote> | |||
'''Discussion''' | |||
1. According to [http://www.sciencedaily.com/releases/2011/09/110927161656.htm Science Daily,] the JAMA “study was a double-blind randomized placebo-controlled clinical trial conducted at 11 North American clinical sites from June 2008 to October 2010. A cohort of 369 men aged 45 years or older participated.” | |||
The group average change in AUASI score [a lower score is better] from baseline to 72 weeks between the saw palmetto and placebo groups was 0.79 points, favoring placebo. Saw palmetto was not more effective than placebo in reducing urinary symptoms for any of the secondary outcomes. | |||
See the JAMA graph below for a more vivid overall description. | |||
<center>http://community.middlebury.edu/~wpeterso/Chance_News/images/CN78_JAMA_graph.png</center> | |||
2. When the results are disaggregated, they appear thusly and the placebo almost always outperforms saw palmetto: | |||
<center>http://community.middlebury.edu/~wpeterso/Chance_News/images/CN78_JAMA_table.png</center> | |||
3. The JAMA article says “1-sided P = .91.” Why was a 1-sided hypothesis test done in place of a 2-sided test? And why is the p-value so ridiculously high? | |||
4. The many clinical studies cited by the Saw Palmetto Trading Company seem to indicate that saw palmetto is effective in treating BPH yet the JAMA article concludes otherwise. Why might the JAMA article be more persuasive than the previous studies? | |||
Submitted by Paul Alper | |||
Revision as of 19:44, 9 October 2011
Quotations
"Data is not information, information is not knowledge, knowledge is not understanding, understanding is not wisdom." -- Clifford Stoll
Submitted by Steve Simon
Forsooth
Cheerful tweets in the morning
Twitter Study Tracks When We Are :) by Benedict Carey, The New York Times, September 29, 2011
If you read the mood of people on Twitter, they are happy in the morning, but then things go downhill.
However grumpy people are when they wake up, and whether they stumble to their feet in Madrid, Mexico City or Minnetonka, Minn., they tend to brighten by breakfast time and feel their moods taper gradually to a low in the late afternoon, before rallying again near bedtime, a large-scale study of posts on the social media site Twitter found.
How can you measure this? The researchers
analyzed the text of each message, using a standard computer program that associates certain words, like “awesome” and “agree,” with positive moods and others, like “annoy” and “afraid,” with negative ones. They included so-called emoticons, the face symbols like “:)” that punctuate digital missives.
It's not an accurate sample, though, as the researchers admit.
For starters, Twitter users are computer-savvy, skew young and affluent, and post for a variety of reasons.
You might think that going to work causes a decline in mood, but the same burst of enthusiasm occurs on Saturday and Sunday mornings, but two hours later than on weekdays. There is, however, no evidence for Seasonal Affective Disorder, the tendency of people to become depressed near Christmas when the days are the shortest. Here's a graph showing the daily trends.
{kind=link}
Submitted by Steve Simon
Questions
1. What aspects of Twitter make you nervous about these findings?
2. Can sentiments like happiness be discovered adequately by text analysis? Does the 140 character limit in Twitter make this more difficult or easier?
Fool’s gold standard
“Buy low, sell high and “avoid trauma” are good aphorisms to live by. So is “never take medication or have a medical procedure performed that has been in use for less than twenty-five years.” And, that is even if said medication or procedure has been approved by the so-called gold standard, a clinical trial. In Chance News 76 one type of what might be called a “fool’s gold standard,” seeding trials, is discussed.
Another version of the fool’s gold standard is the subject of an article entitled The Other South American Drug War, by Kelly Hearn in The Nation (print version to appear 11 October 2011). Hearn describes the subverting of clinical trials by means of “offshoring” clinical trials and Independent Review Boards to South America.
Foreign clinical trials for US-bound drugs have been commonplace for decades, and ethical breaches are a frequent side effect.
A generation ago, most human testing took place in American academic institutions. Now it’s a global game dominated by corporations, called contract research organizations (CROs), that help Big Pharma bring new molecules from the lab to your medicine cabinet. More and more drug companies are turning to CROs for assistance with trial design and recruitment, regulatory compliance, marketing and branding—last year the CRO market was worth $20 billion, an estimated 100 percent jump from a decade ago. And CROs, in turn, are increasingly running trials in the developing world because doing so is cheaper and faster: regulations aren’t as onerous, patient recruitment is easier and informed consent is less clearly defined.
Peru, a nation of 30 million where few people have health insurance and one in three lives in poverty, has the highest number of volunteer patients in South America and ranks among the world’s leaders in total number of clinical trials. In 2008 more than 13,000 Peruvians took part in trials testing drugs intended for the United States. The FDA did not send a single inspector.
It is unnerving to read how easily the system is being gamed.
Discussion
- Hearn quotes someone who states, “A big fear is that reckless researchers or firms may find it easy to go far from regulatory scrutiny and conduct preliminary, early-phase research off the record to find out whether to abandon the idea or to pursue it in the licit, on-the-record procedures.” Why is this a big fear?
- How does number 1 relate to the so-called “file drawer problem of statistics”?
- According to Hearn, “the number of trials in developing countries has grown 8 percent a year since 1997. A 2010 report by the inspector general of the Department of Health and Human Services (HHS) notes that 40 to 65 percent of clinical trials on FDA-regulated products in 2008 took place overseas. Of nearly 6,500 foreign trial sites that year, the FDA inspected only forty-five—less than 1 percent.” If Hearn’s allegations are on the mark, why have we not heard more about them in the mainstream media?
- In the news last month has been criticism of an earlier ethically indefensible use of a clinical trial in Guatemala here.
Submitted by Paul Alper
Saw palmetto and LUTS
As most older men will attest, lower urinary tract symptoms or LUTS in the form of BPH or benign prostatic hyperplasia, is at minimum annoying, and often quite painful. The most common plant extract for treating BPH is the fruit of the saw palmetto dwarf palm tree. Saw palmetto is relatively inexpensive, around 20 to 30 dollars for a so-called month supply and according to The Saw Palmetto Trading Company
Numerous double-blind clinical studies on the Saw palmetto extract have shown it to be effective in nearly 90% of patients usually in a period of 4 to 6 weeks. Detailed toxicity studies in animals, as well as the results from clinical trials, indicate that the Saw palmetto extract is without toxicity or side effect. Despite the impressive clinical effectiveness, safety, and popularity of Saw palmetto extract in the treatment of BPH in the United States, manufacturers are prohibited from making any medical claims by the FDA.
Clinical studies demonstrating the efficacy of Saw palmetto in BPH:
| Authors | Type of Study | No. of patients | Length of study | Results |
|---|---|---|---|---|
| Boccafoschi, et al | Double-blind | 22 | 60 days | Significant difference for volume voided, maximum flow, mean flow, dysuria, nocturia |
| Cirillo,et al | Open | 47 | 4 months | Significant difference for: dysuria, nocturia, urine flow |
| Tripodi, et al | Open | 40 | 30-90 days | Significant difference for: dysuria, nocturia, volume of prostate, voiding rate, residual urine |
| Emili, et al | Double-blind | 30 | 30 days | Significant difference for: number of voidings, strangury, maximum and mean urine flow, residual urine |
| Greca, et al | Open | 14 | 1 to 2 months | Significant difference for: dysuria, perincal heaviness, nocturia, volume of urine per voiding, interval between two dumal voidings, sensation of incomplete voiding |
| Duvia, et al | Controlled trial vs. pygeum | 30 | 30 days | Significant difference for voiding rate |
| Tasca, et al | Double-blind | 30 | 31 to 90 days | Significant difference for: frequency, urine flow measurement |
However, a recent JAMA study indicates that a popular remedy for LUTS might be worthless:
In conclusion, we found that saw palmetto extract used at up to 3 times the standard daily dose had no greater effect than placebo on improving lower urinary symptoms or other outcomes related to BPH.
Discussion
1. According to Science Daily, the JAMA “study was a double-blind randomized placebo-controlled clinical trial conducted at 11 North American clinical sites from June 2008 to October 2010. A cohort of 369 men aged 45 years or older participated.”
The group average change in AUASI score [a lower score is better] from baseline to 72 weeks between the saw palmetto and placebo groups was 0.79 points, favoring placebo. Saw palmetto was not more effective than placebo in reducing urinary symptoms for any of the secondary outcomes.
See the JAMA graph below for a more vivid overall description.
{kind=link}
2. When the results are disaggregated, they appear thusly and the placebo almost always outperforms saw palmetto:
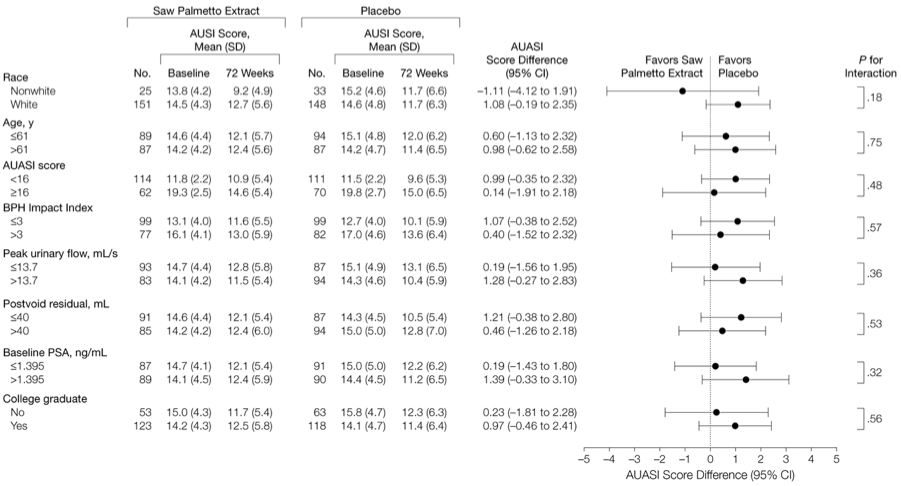{kind=link}
3. The JAMA article says “1-sided P = .91.” Why was a 1-sided hypothesis test done in place of a 2-sided test? And why is the p-value so ridiculously high?
4. The many clinical studies cited by the Saw Palmetto Trading Company seem to indicate that saw palmetto is effective in treating BPH yet the JAMA article concludes otherwise. Why might the JAMA article be more persuasive than the previous studies?
Submitted by Paul Alper